Primary endpoint1
Primary endpoint1
93.5%
(n=29/31, primary efficacy set)
of patients free from protocol-defined severe VOCs for ≥12 consecutive months after infusion with CASGEVY (VF12)*
(98% one‑sided CI: 77.9%, 100.0%)
- At baseline, patients (n=31, primary efficacy set) had a median of 3.5 (range: 2.0-18.5) severe VOCs/year in the 2 years prior to enrollment1
- One VF12 responder, after initially achieving a VF12 response, experienced an acute pain episode meeting the definition of a severe VOC at Month 22.8 requiring a 5‑day hospitalization; this patient was reported to have a parvovirus B19 infection at the time1
Study Design
Trial 1 (NCT03745287) is an ongoing single-arm, multi-center trial evaluating the safety and efficacy of a single dose of CASGEVY in adult and adolescent patients with sickle cell disease. Eligible patients underwent mobilization and apheresis to collect CD34+ stem cells for CASGEVY manufacture, followed by myeloablative conditioning and infusion of CASGEVY. Patients were then followed in Trial 1 for 24 months after CASGEVY infusion. Patients were eligible for the study if they had a history of at least 2 severe VOC events per year in the 2 years prior to screening.1
*The evaluation starts 60 days after last RBC transfusion for posttransplant support or SCD management. Efficacy was evaluated based on interim analysis.1
RBC=red blood cell; SCD=sickle cell disease; VF12=proportion of patients who have not experienced any severe VOCs for at least 12 consecutive months; VOC=vaso-occlusive crisis.
The efficacy and safety profile was generally consistent among pediatric patients aged 12 years and older and adult patients1
The safety and efficacy of CASGEVY has been established in pediatric patients with SCD aged 12 years and older.1
- Use of CASGEVY is supported by data in 12 patients aged 12 to less than 18 years in Trial 1 (6 patients evaluable for the primary efficacy analysis)
- The median (min, max) time to platelet engraftment was 45 (23, 81) days in pediatric patients aged 12 years and older and 32 (23, 126) days in adult patients. The median (min, max) time to neutrophil engraftment was 28 (24, 40) days in pediatric patients aged 12 years and older and 26 (15, 38) days in adult patients
The safety and efficacy of CASGEVY in pediatric patients aged less than 12 years has not been established.1
Key secondary endpoint1
Key secondary endpoint1
100%
(n=30/30, primary efficacy set)
of patients free from inpatient hospitalizations for severe VOCs for ≥12 consecutive months (HF12) after infusion with CASGEVY†
(98% one‑sided CI: 87.8%, 100.0%)
- Of the 31 patients evaluable for VF12 responder status, 1 patient was not evaluable for HF12 responder status1
- At baseline, patients (n=31, primary efficacy set) had a median of 2.0 (range: 0.5-8.5) hospitalizations for severe VOCs/year in the 2 years prior to enrollment1
†The evaluation starts 60 days after last RBC transfusion for posttransplant support or SCD management. Efficacy was evaluated based on interim analysis.1
HF12=proportion of patients free from inpatient hospitalization for severe VOCs sustained for at least 12 months.
Secondary endpoint1-3
Secondary endpoint1-3
22.2
months
(n=29, primary efficacy set;
range: 14.8-45.5 months)
Median duration of protocol-defined severe-VOC-free period of patients who achieved VF12‡
- One VF12 responder, after initially achieving a VF12 response, experienced an acute pain episode meeting the definition of a severe VOC at Month 22.8 requiring a 5-day hospitalization; this patient was reported to have a parvovirus B19 infection at the time1
- The range is not included in the full Prescribing Information and is presented for descriptive purposes only.
‡The evaluation starts 60 days after last RBC transfusion for posttransplant support or SCD management. Efficacy was evaluated based on interim analysis.1
Secondary endpoint1,2
Secondary endpoint1,2
Increased mean HbF levels to
>40%
at Month 6
Sustained HbF levels >40% through
Total Hb and HbF proportion1
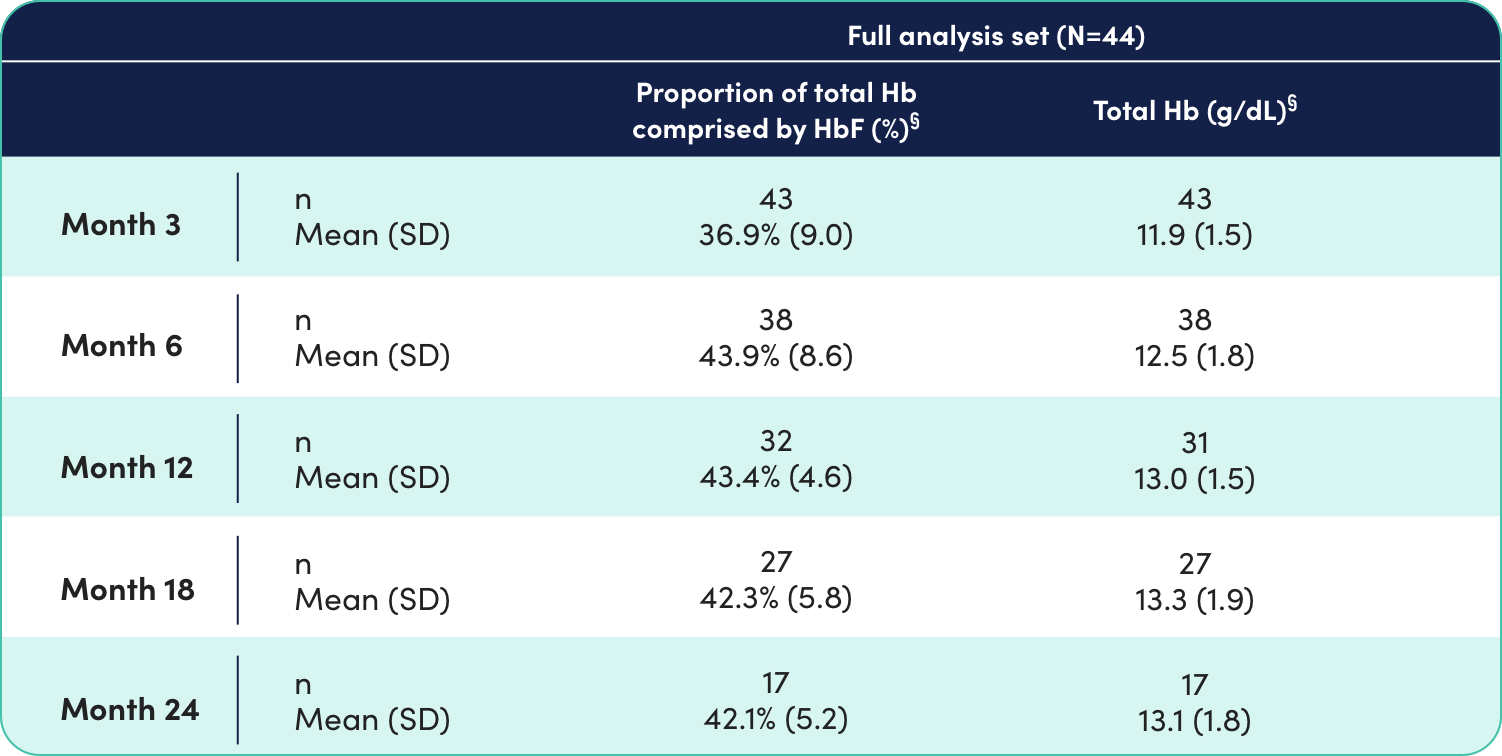
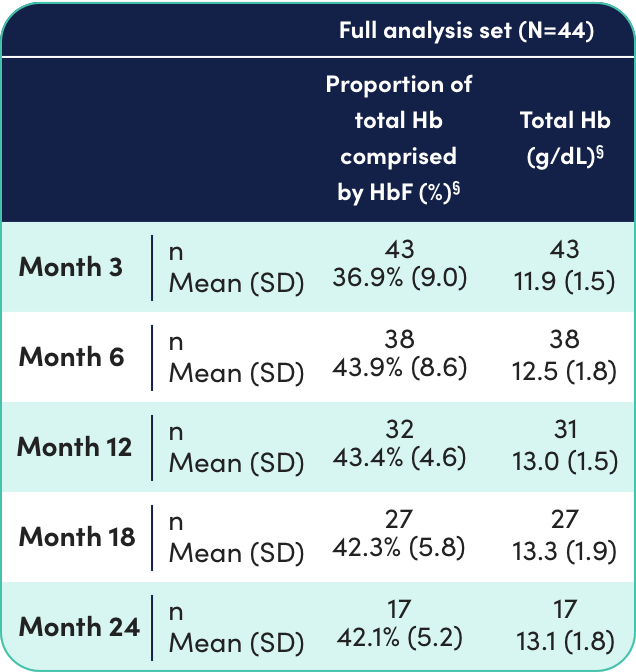
Of the 44 patients infused with CASGEVY, 3 male patients reached total Hb levels of at least 16.5 g/dL at one or more timepoints after Month 9.1
§%HbF/Hb data not available for all patients at all timepoints.1
Consistent with the increase in HbF levels, the proportion of F cells continued to increase until Month 6 and remained stable thereafter, indicating sustained pancellular expression of HbF.1
Total Hb and HbF over time in Trials 1 and 34


Data are not included in the full Prescribing Information and are presented here for descriptive purposes only.
BL=baseline; F cells=circulating erythrocytes expressing HbF; Hb=hemoglobin; HbF=fetal hemoglobin; SD=standard deviation; SE=standard error.
Secondary endpoint1-3
Secondary endpoint1-3
Durable BCL11A editing was achieved in bone marrow (CD34+ cells) and peripheral blood (nucleated cells) through Month 24
Results show proportion of alleles with intended genetic modification in CD34+ cells in bone marrow over time1||
Results by patient are not included in the full Prescribing Information and are presented here for descriptive purposes only. Each line represents an individual patient.3
Full analysis set (N=44)1,3


||Allelic editing data not available for all patients at all timepoints.1
Results show proportion of alleles with intended genetic modification in peripheral blood over time.1
Results by patient are not included in the full Prescribing Information and are presented here for descriptive purposes only. Each line represents an individual patient.3
Full analysis set (N=44)1,3


IMPORTANT SAFETY INFORMATION
WARNINGS AND PRECAUTIONS
Neutrophil Engraftment Failure
Monitor absolute neutrophil counts (ANC) and manage infections according to standard guidelines and medical judgement. In the event of neutrophil engraftment failure, patients should be infused with rescue CD34+ cells.
Delayed Platelet Engraftment
Delayed platelet engraftment has been observed with CASGEVY treatment. There is an increased risk of bleeding until platelet engraftment is achieved. In the clinical trials, there was no association observed between incidence of bleeding events and time to platelet engraftment.
Monitor patients for bleeding according to standard guidelines and medical judgement. Conduct frequent platelet counts until platelet engraftment and platelet recovery are achieved. Perform blood cell count determination and other appropriate testing whenever clinical symptoms suggestive of bleeding arise.
Hypersensitivity Reactions
Hypersensitivity reactions, including anaphylaxis can occur due to dimethyl sulfoxide (DMSO) or dextran 40 in the cryopreservative solution. Monitor patients for hypersensitivity reactions during and after infusion.
Off-Target Genome Editing Risk
Although off-target genome editing was not observed in the edited CD34+ cells evaluated from healthy donors and patients, the risk of unintended, off-target editing in an individual’s CD34+ cells cannot be ruled out due to genetic variants. The clinical significance of potential off-target editing is unknown.
ADVERSE REACTIONS
The most common Grade 3 or 4 non-laboratory adverse reactions (occurring in ≥ 25%) were mucositis and febrile neutropenia in patients with SCD and patients with TDT, and decreased appetite in patients with SCD.
All (100%) of the patients with TDT and SCD experienced Grade 3 or 4 neutropenia and thrombocytopenia. Other common Grade 3 or 4 laboratory abnormalities (≥ 50%) include leukopenia, anemia, and lymphopenia.
DRUG INTERACTIONS
No formal drug interaction studies have been performed. CASGEVY is not expected to interact with the hepatic cytochrome P450 family of enzymes or drug transporters.
Use of Granulocyte-Colony Stimulating Factor (G-CSF): G-CSF must not be used for CD34+ HSC mobilization of patients with SCD.
Use of Hydroxyurea: Discontinue the use of hydroxyurea at least 8 weeks prior to start of each mobilization cycle and conditioning. There is no experience of the use of hydroxyurea after CASGEVY infusion.
Use of Voxelotor and Crizanlizumab: Discontinue the use of voxelotor and crizanlizumab at least 8 weeks prior to start of mobilization and conditioning, as their interaction potential with mobilization and myeloablative conditioning agents is not known.
Use of Iron Chelators: Discontinue the use of iron chelators at least 7 days prior to initiation of myeloablative conditioning, due to potential interaction with the conditioning agent. Some iron chelators are myelosuppressive. If iron chelation is required, avoid the use of non-myelosuppressive iron chelators for at least 3 months and use of myelosuppressive iron chelators for at least 6 months after CASGEVY infusion. Phlebotomy can be used instead of iron chelation, when appropriate.
USE IN SPECIFIC POPULATIONS
Pregnancy/Lactation: CASGEVY must not be administered during pregnancy and breastfeeding should be discontinued during conditioning because of the risks associated with myeloablative conditioning. Pregnancy and breastfeeding after CASGEVY infusion should be discussed with the treating physician.
Females and Males of Reproductive Potential: A negative serum pregnancy test must be confirmed prior to the start of each mobilization cycle and reconfirmed prior to myeloablative conditioning.
Women of childbearing potential and men capable of fathering a child should use effective methods of contraception from start of mobilization through at least 6 months after administration of CASGEVY. Advise patients of the risks associated with conditioning agents.
Infertility has been observed with myeloablative conditioning therefore, advise patients of fertility preservation options before treatment, if appropriate.
Please see full Prescribing Information for CASGEVY.
References: 1. CASGEVY [prescribing information]. Vertex Pharmaceuticals Incorporated. Boston, MA; January 2024. 2. Protocol for: A phase 1/2/3 study to evaluate the safety and efficacy of a single dose of autologous CRISPR-Cas9 modified CD34+ human hematopoietic stem and progenitor cells (CTX001) in subjects with severe sickle cell disease. Vertex Pharmaceuticals Incorporated. Boston, MA. September 2021. 3. Frangoul H, Locatelli F, Sharma A, et al. Exagamglogene autotemcel for severe sickle cell disease. Presented at: American Society of Hematology Annual Meeting and Exposition; December 11, 2023; San Diego, CA. 4. Supplement to: Frangoul H, Locatelli F, Sharma A, et al. Exagamglogene autotemcel for severe sickle cell disease. N Engl J Med. 2024;390(18):1649-1662. doi:10.1056/NEJMoa2309676